











- Gender
- Female
- Age
- 22
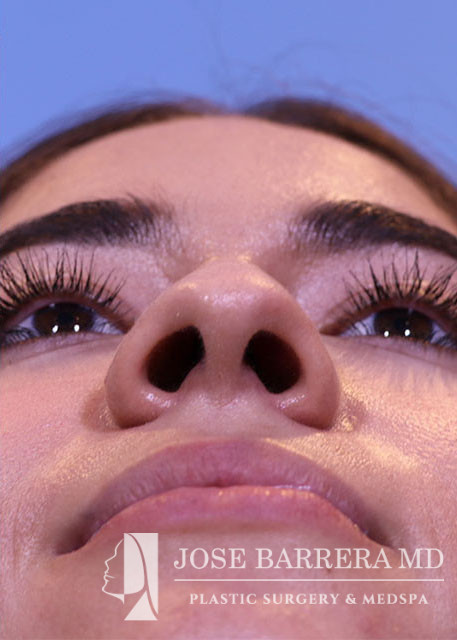
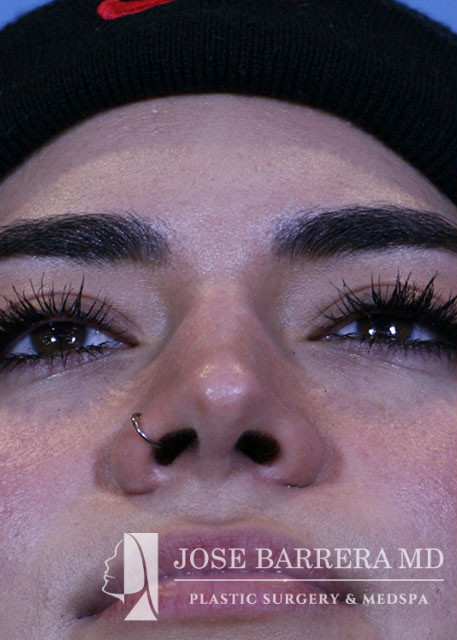
Description
The patient is 2 years postop from her Cosmetic septorhinoplasty. She doesn’t like how her nose goes down when she smiles. She would like to have a slope to her nose. She denies issues with nasal breathing. An inverted V columellar incision and marginal incisions were marked out and incised. The soft tissue envelope was lifted off the cartilage and bony framework. Periosteum over nasal bones incised and subperiosteal plane was dissected.An incision was then made along the pyriform aperture and the skin and soft tissue was elevated off the maxilla and nasal bones to prepare for osteotomies. Low-low-high osteotomies were performed using the Piezo and osteotome. The nasal bones were infractured to narrow the dorsum.The medial crura were separated sharply. The anterior septal angle was identified. A left mucoperichondrial flap was elevated. Dissection proceeded anteriorly around the caudal end of the septum allowing elevation of a mucoperichondrial flap on the right. Septal cartilage was harvested with care taken to maintain greater than 1 cm L strut. The cartilage was used to fashion a septal extension graft. Additionally, the bony septum was found to be deviated and so it was removed.Cephalic trims were performed leaving 8mm wide lower lateral cartilages. The septal extension graft was secured to the right side of the native septum with 5-0 prolene. A small buttressing graft was fashioned from patient’s native septal cartilage and secured to the left side of the septum with 5-0 prolene. 5-0 prolene dome spanning and lateral crural tensioning sutures were placed to create new domes and increase rotation, securing the lower lateral cartilages to the septal extension graft. The skin was elevated off the medial crura. A partial tongue-in-groove procedure was performed and the medial crura were sutured to the caudal septum with 5-0 prolene. Medial crural fixation sutures were placed to secure the medial crura together and narrow the columella.
