
























- Gender
- Female
Description
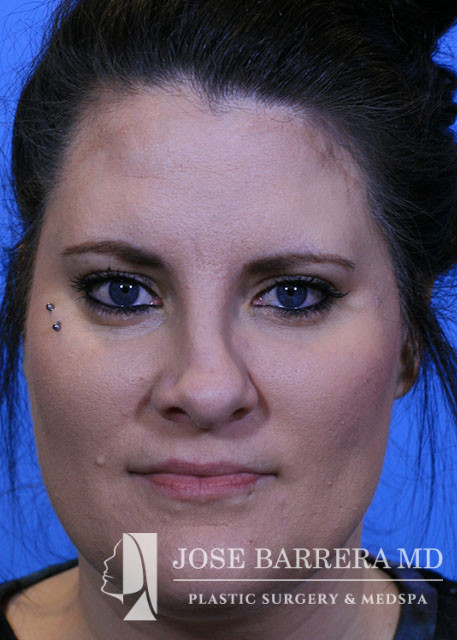
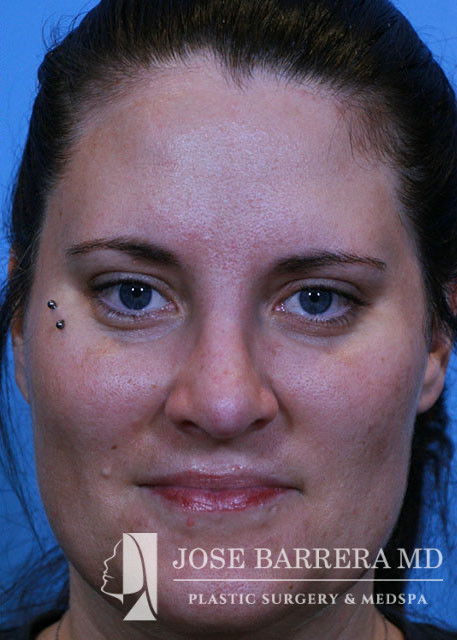
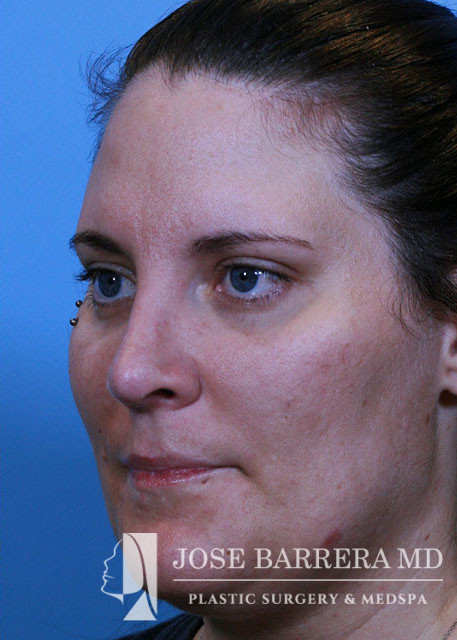
Operation: 34 yo female who underwent Revision Preservation Rhinoplasty, with Cottle SPAR B technique, Right SEG, Costal Cartilage Grafting. Asymmetric LLH osteotomies with a low strip taken on the right and no strip on the left.
Indications:
Description of procedure:
Pre-operative diagnosis:
Aesthetic nasal concerns
Post-operative diagnosis:
Aesthetic nasal concerns
Procedure:
1. Revision preservation open septorhinoplasty – Modified Cottle / SPAR B
2. Costal cartilage grafting – SEG
Findings:
The patient had previous septoplasty and subsequent nasal trauma within 1 week of her operation. This left her with a severely twisted septum that distorted the midvualt and tip with deviation to the left and right sidewall depression. After her nose was open there was evidence of cephalic trim to the LLC. This suggested previous rhinoplasty. The nasal dorsum was intact and there was no evidence of grafting.
Procedure:
The patient was brought to the operating room and identified by name and date of birth. Intravenous anesthesia was administered and an LMA was placed. The nose, pyriform and septum were infiltrated with 1% lidocaine with 1:100,000 epinephrine. The patient was prepped and draped in the standard sterile fashion.
An inverted V columellar incision and marginal incisions were marked out and incised. The soft tissue envelope was lifted off the cartilage and bony framework. The periosteum over the nasal bones was incised and elevated.
An incision was then made along the scroll region and the skin and soft tissue were elevated off the maxilla and nasal bones to prepare for osteotomies. The Piezo saw was then used to make low-low-high osteotomies as well as a horizontal osteotomy at the nasion. The dorsal roof remained intact. Small segments of nasal bone were removed at the pyriform aperture to allow for let down and correction of axis deviation but only on the right side.
The medial crura were separated sharply. The anterior septal angle was identified. A left mucoperichondrial flap was elevated. Dissection proceeded anteriorly around the caudal end of the septum allowing elevation of a mucoperichondrial flap on the right. There was previous cartilage resection. The high septum was severely deviated and there was a cartilaginous spur at the junction with the PPE. This was shaved flush with the septum. There was twisting of the caudal septum and the septum was deviation off of the maxillary crest. We elected to perform a Cottle/Spar B approach to correct this deformity. the caudal septum was released from the nasal spin and maxillary crease. The cartilaginous septum was released from the PPE. An osteotomie through the PPE was made connecting with the transvers osteotomy.
