
























- Gender
- Female
- Age
- 25
Description
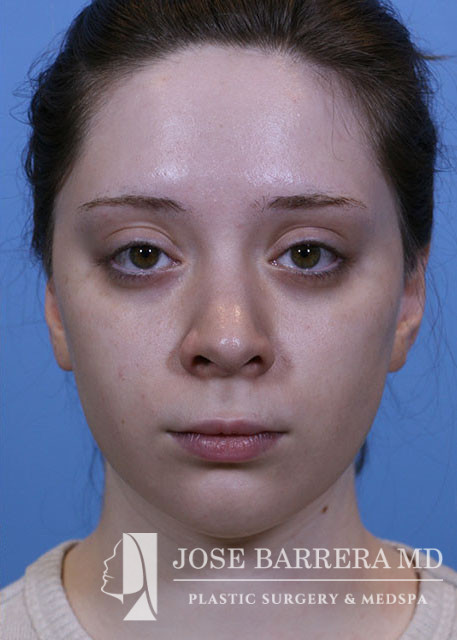
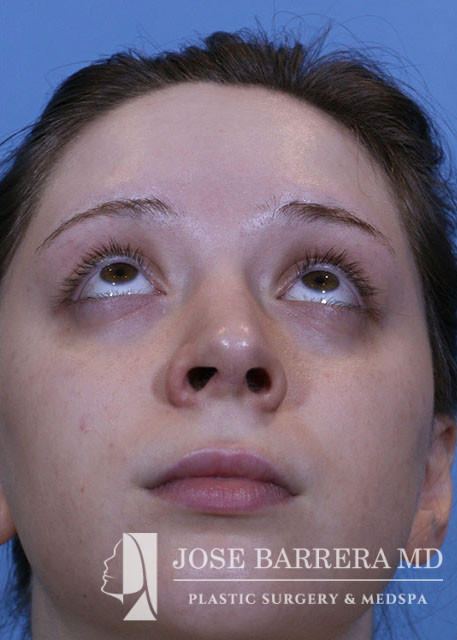
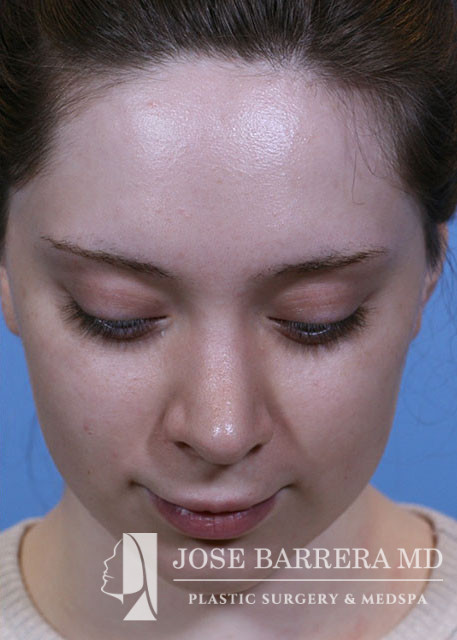
Operation: Primary Preservation Rhinoplasty, Z Flap, Left SEG, Crushed Cartilage supratip graft. Submental Liposuction
Indications:
Description of procedure:
Pre-operative diagnosis:
1. Aesthetic nasal concerns
2. Submental fat pad hypertrophy
Post-operative diagnosis:
1. Aesthetic nasal concerns
2. Submental fat pad hypertrophy
Procedure:
1. Primary preservation open septorhinoplasty
2. Septal cartilage grafting
3. Submental Liposuction
Procedure:
The patient was brought to the operating room and identified by name and date of birth. Intravenous anesthesia was administered and an LMA was placed. The nose, pyriform and septum were infiltrated with 1% lidocaine with 1:100,000 epinephrine. The patient was prepped and draped in the standard sterile fashion.
An inverted V columellar incision and marginal incisions were marked out and incised. The soft tissue envelope was lifted off the cartilage and bony framework. The periosteum over the nasal bones was incised and elevated.
An incision was then made along the scroll region and the skin and soft tissue were elevated off the maxilla and nasal bones to prepare for osteotomies. The Piezo saw was then used to make low-low-high osteotomies as well as a horizontal osteotomy at the nasion. The dorsal roof remained intact. Small segments of nasal bone were removed at the pyriform aperture to allow for let down of the dorsal hump.
The medial crura were separated sharply. The anterior septal angle was identified. A left mucoperichondrial flap was elevated. Dissection proceeded anteriorly around the caudal end of the septum allowing elevation of a mucoperichondrial flap on the right.
Next, a modified through and through dorsal cartilage z plasty incision was performed along with an osteotomy through the perpendicular plate of the ethmoid bone to allow for let down of the dorsal hump. At this point, the nasal dorsum was fully let down. A 5-0 prolene was placed around the excised septal cartilage segment to hold the let down dorsal hump in position. An inferior oblique incision is then carried caudally through to the anterior septal angle to level of cartilaginous dorsum.
